The app and website was publicly released on 2 Apr 2024
Update Jan 2025
The content continues to undergo review by all our cadres.
The content remains subject to the following provisos: - The content will be subject to continuous update and review - Old content (from previous CGOs) will be converted into the new format, using the new tools and layouts - Content may be moved around - The layout will change and reflect the needs of the user - Content will be created - Content may be deleted/retired
CGO development will continue.
Saf [Updated 21 Jan 2025]
Deployed General Anaesthesia
!Warning
What's new / Latest updates
Transitioned into new format (from PDF/JPGs).
Removed references to brand names for equipment - eg Video laryngoscope rather than Glidescope
Amended SI units to reflect current practice
Objectives
This guideline is designed to support clinicians within their deployed scope of practice provide general anaesthesia. It aims to provide a safe and reasonable approach, recognising that clinical teams will provide tailored care depending their experience, training, operational constraints and the presenting patient. Multiple activities are likely to be performed by the anaesthetic team, these areas have their own guidelines and for the sake of brevity have been de-emphasised here.
Scope
What preparation should be done prior to casualty arrival?
What equipment might be needed for an RSI in different locations?
What drugs might be used during an RSI in different situations?
What are the considerations for the anaesthetist during damage control surgery?
What different communication tools can be used before and during damage control resuscitation/surgery?
What different strategies can be used for specific clinical problems?
Audience
Anaesthetists
Peri-operative practitioners
Emergency medicine physicians
Emergency department nurses
Pre-hospital practitioners
Initial Assessment & Management
Before the casualty arrives
Assess (9 Liner / MISTAT)
Number, type and severity of casualties?
Airway at risk or already secured?
Likely to need massive transfusion?
Ongoing or concurrent - clinical and operational?
Anticipate
Consider likely casualty flow (within and beyond the facility)
Consider potential courses of action and brief medical teams
Determine need to split team between casualties / clinical areas
Remember - temperature / acidosis / calcium / coagulopathy
Prepare equipment
Airway equipment, oxygen, suction, ventilator
Anaesthetic drugs (consider pre-made "wet packs")
Prioritise large bore venous access - consider invasive lines
Environmental considerations - patient warming and pressure care
Damage control resuscitation - anaesthetic considerationsDamage control resuscitation requires concurrent and coordinated activity from the whole team. This process will likely be lead by the emergency physician initially. Exact roles will be determined by clinical priorities and team composition. Coordination with the clinical director and facility OC is essential to maintain situational awareness for appropriate planning.
Catastrophic Haemorrhage
Identify (including early exposure and roll) and stop the bleed. If external control of ongoing catastrophic bleeding impossible, all efforts should be directed at immediate surgical control of bleeding. This may require induction of anaesthesia in an unstable patient - adjust drug doses, ventilation and fluids accordingly. Consideration should be given as to the appropriate location for induction of anaesthesia.
Airway
See airway guidelines. Oxygenation is the priority at all times. Asses airway and placement of adjuncts, capnography is advised when airway adjuncts are placed and mandated following tracheal intubation. Take a view on likely course and potential for deterioration given location and onward care. Basic airway manoeuvres (including postural changes), devices (including a pillow) and suction may temporise threatened airways. An obstructed or unsafe airway maybe an indication for urgent RSI.
Breathing
Administer high flow oxygen in the critically ill patient, in everyone else titrate (94-98%). Multi-modal analgesia will assist with chest drain insertion and may improve ventilation. Respiratory distress may be an indication for RSI. In severe hypovolaemic shock, aim to minimise intra-thoracic pressure during positive pressure ventilation.
Circulation
Critical / emergency care is largely impossible without IV / IO access, the anaesthetist is well placed to assist in its placement. Prioritise large bore venous access either peripheral or central, consider use of ultrasound to assist. Aim to administer a balanced transfusion if ongoing haemorrhage. Anticipate coagulopathy - address low temperature, low calcium and acidosis. Aim for haemostatic resuscitation, try to avoid shock, consider fresh whole blood and use of adjuncts including TXA / fibrinogen. Be guided by primarily by physiological parameters in the hyper acute phase. Point of care testing, including blood gas and coagulation assays are informative but take time to process, as a result they may delay active treatment and will often be behind the curve.
Disability and distress
See analgesia and sedation guidelines. RSI may be indicated if GCS is reduced. If induction of anaesthesia has been performed maintain anaesthesia usually with an IV agent and ideally via a pump. Ready the patient for onward transfer.
Environment / everything else
Expose the patient and consider the need for further examination, either to complete initial survey or to review following interventions to track progression. Maintain dignity, hygiene and aim for normothermia. Review investigations. Complete documentation and ensure accurate prescriptions.
The command huddle
Periodically a pause to share findings, decision-making and predicted trajectory is important. The commonly termed a "command huddle" allows the clinicians responsible for care to maintain situational awareness and maintain the tempo of care. In smaller teams it is often appropriate for all members to be included in these reviews.
Advanced Assessment & Management
Rapid Sequence Induction (RSI)
It is likely that deployed general anaesthesia will be be required for unscheduled or emergency care. Within the wider clinical team, "RSI" is synonymous with emergency anaesthesia, an intervention undertaken to provide critical care or facilitate surgery. Clinicians should remember the considerable additional demands on the operational patient pathway demanded by the anaesthetised patient and should explore alternatives wherever practicable (procedural sedation / regional anaesthesia / delayed treatment etc).
While the components of an RSI have changed over the years the clinical objectives have not. Clinicians still aim to induce anaesthesia and secure the airway whilst reducing the risk of pulmonary aspiration. Consideration however must also be given to the other potential risks including but not limited to: difficult airway, cervical spine injury, hypoxia, hypercapnia and cardiovascular compromise.
The approach to deployed anaesthesia should be pragmatic and tailored to the patient and situation. Deployed anaesthesia, even for routine cases is a high consequence, low frequency intervention. The anaesthetic team should seek to anticipate, communicate and mitigate concerns.The safest course of action is likely to be that which is most familiar to the clinical team present.
Indications
Indications for RSI in the resus bay:
Compromised airway eg facial trauma
Inadequate ventilation eg pneumonia
Low GCS or agitation eg head injury
Humanitarian eg uncontrollable pain
Anticipated deterioration - eg facial burn
Indications for RSI on the operating table:
Anticipated high aspiration risk eg emergency surgery
RSI in uncontrolled intra-abdominal (or other cavity) bleeding may be more appropriate on the operating table, immediately prior to surgery.
Equipment and Team
Equipment should include:
BVM or Mapleson C (Water's) with appropriate mask
Yankauer suction (consider NGT / drain)
2 sizes of working laryngoscope (including VL)
Appropriately sized ETT (+ 1 size below) and lubricant
Bougie (consider 1st line)
End-tidal CO2 (ideally waveform)
Catheter mount and HMEF
Syringe and tube tie / tape
Pillow or positioning aid
Difficult airway - (OPA / NPA / SGA / X-blade and stylet / bronchoscope and Aintree)
Can't oxygenate - No 10 scalpel / 6mm ETT
Team should include (+potential actions):
Anaesthetist - airway lead
Experienced anaesthetic assistant
2nd clinician to give drugs and monitor cardiovascular changes
Team leader made aware prior to RSI and present to coordinate emergency actions eg thoracostomy in case of tension pneumothorax, blood transfusion in case of CVS compromise
Induction drugs
In major trauma these drugs are routinely used. Discussion of pharmacokinetic / pharmacodynamic discussion is beyond the scope of this guideline.
Preferred agents
Fentanyl 1-2μg/kg at induction. Short acting analgesic, may obtund hypertension of laryngoscopy. Consider higher doses in isolated head injuries. Caution in hypovolaemia, consider omitting or lowering the does.
Ketamine 1-2mg/kg. More cardio stable than propofol. Analgesic and sedative properties depending on dose. Likely to precipitate a tachycardia.
Rocuronium 1mg/kg. Preferred paralysing agent. Intubating conditions at one minute, may be slower if low cardiac output. Painful on injection. Stable at STP for 90 days.
Propofol 2 mg/kg or using TCI algorithm, caution in hypotension
Points to consider:
Hypovolaemia
In order to control haemorrhage surgery and therefore anaesthesia may be required prior to optimisation. Shocked patients are demonstrate a greater neurological (relatively conserved cerebral blood flow) and cardiovascular (low protein binding following resuscitation, often under-filled, dependent on sympathetic drive) sensitivity to anaesthetic agents; consider dose reductions. Induction agents with a high therapeutic index are preferred to reduce risks of awareness and haemodynamic compromise. Following induction, positive pressure ventilation will likely reduce cardiac filling in hypovolaemia and tamponade, and may precipitate tension pneumothorax.
Consider fentanyl or ketamine to control agitation (DSI) and facilitate optimisation.
Where practical, correct hypovolaemia prior to RSI; if impractical ensure ongoing volume resuscitation
Consider reduced drug dosing including omission of opiates.
Allow for delayed onset time (reduced cardiac output)
Reduce tidal volume and PEEP (to increase cardiac filling).
Aim for radial pulse if uncontrolled bleeding, aim for normal BP once surgical control
Treat hypovolaemia with volume and treat vasoplegia with pressors
Patient positioning and ramping
Patient positioning is challenging when care is provided on a stretcher. Civilian style trollies are likely a better option if available to optimise positioning for airway management and oxygenation. The operating table allows for a degree of tilt that may facilitate pre-oxygenation or postural drainage. Additional equipment including blankets and pillows may be used to provide an pragmatic solution. Elevating stretcher back rests are available but are not easily re-positioned. Positioning for airway trauma is anticipated to be difficult when patients may prefer to be sitting prior to induction of anaesthesia, the use of additional personal to offer physical support or induction on the floor have both been described.
C-Spine Precautions
Recent (2024) UK guidance from the Association of Anaesthetists recommends that in cases of potential cervical spine injury; attempts should be made to minimise neck movement during pre-oxygenation and facemask ventilation. If a simple manoeuvre is required to maintain an airway a jaw thrust is advised. Videolaryngoscopy is recommended and clinicians should be competent in its use. An adjunct (stylet or bougie) should be considered when performing tracheal intubation. Cervical collars should be removed or loosened during laryngoscopy. A pragmatic "all-risks" approach, to mitigating against unnecessary cervical spine movement is recommended.
Cricoid pressure
Application of cricoid pressure has been demonstrated to hamper laryngoscopy and increase cervical spine movement. However the most recent (2015) DAS RSI guideline still recommend its application, ie 10 N (1 kg) when the patient is awake, increasing to 30 N (3 kg) upon loss of consciousness, to be removed only if active vomiting occurs or to improve oxygenation and intubation. PUMA currently include cricoid as a optional component of RSI. The 2025 pre-hospital guidelines from the Association of Anaesthetists (UK) are equivocal but point to a poor evidence base of efficacy, risk of harm and absence from European guidelines. A pragmatic "all-risks" approach, to mitigating against aspiration of gastric contents is recommended.
Pre-oxygenation
While pre-oxygenation is possible to achieve using a ventilator, most clinicians would advocate using a separate method of oxygen delivery to facilitate de-nitrogenation; either a "trauma" mask (with reservoir, 15 l/pm), a Mapleson C Circuit (Water's) or a BVM. This approach is likely to be more in keeping with regular practice, is simpler and less likely to result in error or delay.
VL or DL
In UK civilian practice VLS is increasingly becoming the fist line device for intubation. The deploying anaesthetist must be familiar with the devices available on in their facility. In cases of anticipated difficulty or airway trauma the VLS may allow the wider team to visualise the airway. Use of an adjunct (eg stylet) is recommended, especially when difficulty is anticipated or when using a hyper angulated blade.
TIVA or Volatile
Total Intra Venous Anaesthesia is growing in popularity in UK practice. There are several features of TIVA that make it appealing to deployed anaesthesia - reduced equipment, uninterrupted induction, maintenance of anaesthesia and onward sedation and clinical familiarity. If using TIVA, clinicians should consider the guidance from the Association of Anaesthetists that states processed EEG should be used when TIVA is administered together with a neuromuscular blocker. During emergency surgery for patients requiring volume resuscitation compartment model predictions are likely to be unreliable.
DMS pumps models include Marsh, Schneider (Propofol) and Minto (Remifentanil). Other protocols have been described for use in the deployed environment but are clearly more limited in their evidence base. Continuous infusion of Ketamine for sedation following induction of anaesthesia is well described in prehospital care (military and civilian). A recent scoping review "found a lack of high-quality well-designed studies investigating the use of continuous ketamine sedation on ICU. The available data suggests this intervention is safe and well tolerated, however this is of very low certainty given the poor quality of evidence."
TIVA for War Surgery (Lewis S, Jagdish S, Total Intravenous Anaesthesia for War Surgery BMJ Military Health 2010;156:S301-307)
Inhalational induction
Sevoflurane is the ideal volatile agent for inhalational induction. In the deployed environment this technique is usually likely going to be used for uncooperative or anxious child or those with difficult venous access. The major hazards associated with inhalational induction include the uncooperative child, loss of the airway and laryngospasm. A full stomach, low cardiac output state and a compromised airway are relative contraindications. Sevoflourane may either be incrementally increased or for faster induction the induction setting on the Diamedica Draw-over Vaporiser (DDV2) will deliver in excess of 7-10% (at 20-30 deg C internal temperature). It is common practice to maintain a high inspired volatile concentration until i.v. access is gained, and the return to baseline heart and respiratory rate - useful indicators of adequate depth of anaesthesia whereby insertion of airway adjuncts or cannulation should not provoke laryngospasm. Full anaesthetic monitoring should be applied once the child is anaesthetised.
Checklists
Checklists are used frequently by anaesthetists to improve safety. Checklists help to reduce error, improve consistency and maintain safe systems of work. Widely adopted relevant examples include: equipment checklists published by the Association of Anaesthetists, RSI checklists published by the RCOA, Faculty of Intensive Care and the Surgical Safety Checklist instituted by the WHO. Checklists currently used in deployed perioperative care include the WHO surgical safety check list (full or SNAP) and the sit-rep, encompassing the STACK (Systolic, Temperature, Acidosis, Clotting, Kit). The MERT prehospital anaesthesia SOP includes a pre-RSI checklist. Consideration should be given to the local adoption of bespoke checklists, especially for low frequency high impact clinical interventions.
In the Operating Room
Positioning on Arrival in the Operating Room
Crucifix - The default patient position is Supinewith both arms abducted on boards. Consider potential pressure areas (including occiput) and mitigate accordingly. Protect the eyes.
Apply forced air warmer/under warmer, and commence warming ASAP. Consider invasive temperature monitoring to guide warming.
Don't attempt an arterial line until a strong radial pulse is palpable. Consider urinary catheterisation early. If not already inserted consider CVC for ongoing care.
Handover from the Trauma Team Leader
Handover begins when the patient is properly positioned and safely established on the ventilator / anaesthetic and full monitoring has been applied. Information should include:
Team introduction if any new members.
Introduction to patient (ATMIST may be repeated)
Summary of findings
Treatments given so far
Transfusion running totals
Outstanding issues / tasks / medications
Provisional surgical plan
Post op plan
Maintenance of Anaesthesia
During hypovolaemic shock, titrate fentanyl and volatile / TCI anaesthetic agents carefully. The priority is haemodynamic resuscitation and survival.
When bleeding is controlled, carefully titrate in further analgesia (e.g. consider fentanyl up to 15μg/kg) to reduce sympathetic tone, prevent excessive vasoconstriction and permit further volume resuscitation with blood products.
Consider how multimodal analgesia (including regional anaesthesia) may be be implemented to improve comfort, reduce stress and aid onward transfer.
Haemostatic Resuscitation
Prior to surgical control blood transfusion will likely be balanced ie 1:1 (RBC:FFP). Maintain circulating volume with blood products as per the UK Military Massive Transfusion Protocol. Depending on staffing it may be appropriate to devolve anaesthetic roles roles, separating airway interventions / anaesthesia from blood administration / resuscitation. After surgical control has been achieved and there is a degree of physiological stability a single anaesthetist may perform all these roles. During damage control resuscitation beware over-transfusion and hyperkalaemia. As resuscitation continues it is appropriate to Move from a balanced to a tailored transfusion, guided by physiology and lab tests, including blood gas analysis and viscoelastic testing. Be wary of: hyperkalaemia, hypocalcaemia, hypothermia, acidosis and evolving coagulopathy.
Non Technical Skills - Communication and Teamworking
Leadership, followership, teamwork, and situational awareness and communication amongst the team are all vital to ensure safe care.
Maintain effective 2-way communication with Surgery, Radiology, Critical Care and the Deployed Medical Director (if present).
The WHO CHECKLIST (or abridged DCS snap brief should be used before every case, an aide memoir can be found on the theatre documentation.
A sit rep including time check, STACK (Systolic Temperature, Clotting and Kit), and surgical plan can be considered every 10-30 minutes, after 2+2 blood transfusion or whenever deemed appropriate. These short re-caps help to maintain whole team situational awareness and assist with dynamic decision making. Surgical teams are likely to be focused while operating; plans for onward transfer, time constraints and resource limitations need to be communicated in a considerate fashion. Clinical concerns should be raised early and especially if regarding a patients physiological status is deteriorating.
Encourage and facilitate passage of key information from surgeons, especially:
Release or application of tourniquets, vascular clamps or endovascular occlusive
Difficult surgical control of haemorrhage
Surgical evidence of coagulopathy
Changes in surgical findings or plan
Remember the Deployed Medical Director for: - Activation of the Emergency Donor Panel - Requests for transfer out of the facility - Difficult futility decisions - Resolution in areas of disagreement
Preparing for Post-operative Care
Agree next destination (e.g. critical care, aeromed or CT [where available])
Ensure effective post-operative analgesia, including systemic analgesics and regional anaesthesia
Handover to the receiving team
Prolonged Casualty Care
See critical care
Paediatric Considerations
The Association of Paediatric Anaesthetists provides a comprehensive learning resource: Paediatric Anaesthesia for Beginners online which may serve a useful aide memoir.
In the context of deployed paediatric anaesthesia, care for the very small, chronically ill or complex patient is unlikely to be encountered. Most paediatric patients that have been cared for by the DMS are otherwise well children who have suffered injury. Refer to the paediatric section of CGOs for general guidance. The published age per age section should be used instead of relying on drug calculations. Age per page calculations are largely based on western children and use ideal body weights. If age is unknown or there is a disparity between a patients age and predicted weight defer to the page representing actual weight rather than age (anticipating that it is most likely for patients to be under rather than over predicted weights). Double check unfamiliar doses and consider drawing up required doses into smaller syringes rather than titrating from larger.
Premedication:
Oral midazolam 0.5 mg/kg (up to 10mg) may be helpful when managing the anxious child.
Short procedures may be performed using only an induction dose of ketamine (2 mg/kg)
Avoid propofol for maintenance of anaesthesia unless no other option exists.
Mapleson F Breathing system
Also known as a Jackson-Rees modification to the Ayre’s T-piece is a low resistance and low dead space system. It can be used for spontaneous, assisted and controlled ventilation in all ages although is inefficient >20kg. Flows should be 3 x minute volume (4 l/min minimum flow). PEEP / CPAP is provided by partially occluding end of the bag. Scavenging is inefficient.
Notes on neonates and infants
More sensitive to anaesthetic drugs and less protein binding - lower doses required per kg.
More prone to desaturation - lower FRC
More prone to apnoea and bradycardia - age related, worse if hypoxic, hypercarbic, acidotic
More prone to hypoglycaemia and hypothermia - check temperature and blood sugar regularly.
Small airways - consider a roll under the shoulder and remember neutral positioning.
Thermoregulation
Children are prone to hypothermia
Thermoregulation is a significant metabolic stressor
Monitor temperature frequently (ideal constantly)
Maintain normothermia aggressively
Use warm fluids
Keep covered where possible
Use multimodal warming wherever possible.
Endobronchial intubation
Tracheal tube size should be based on the age per page calculations or estimates from the diameter of the child’s nostril or little finger. A term infant will usually require a 3mm micro cuff tube, alternatively; internal diameter for an uncuffed tube = (age / 4) + 4. Reduce the sized by 0.5mm for micro cuffed tubes. Expected tube length at the lips (age/2 + 12).
To avoid subglottic damage ensure the tube passes easily.
Beware endobronchial intubation, especially after movement or postural change, listen carefully in both axilla.
Fix ETT securely, the trouser leg tape method is used to good effect.
Anticipated Difficult Airway
Thankfully these are uncommon. Remember good communication and utilisation of the whole team. The step wise principles are similar to those in adult practice. CICV – options will depend on surgical expertise, it is unlikely that those present will be familiar with emergency paediatric tracheostomy.
Needle cricothyroidotomy is the preferred first option. (Extend the neck using a shoulder roll, stabilise larynx with non-dominant hand, access the cric membrane with 14 or 16G cannula, aim in a (cordad) direction, confirm location by aspirating air. Connect to either an adjustable pressure limiting device or a 4 Bar O2 source with flow meter (set l/m to child’s age via a Y connector. 1:4 (inspiration : expiration). Cautiously titrate pressure to achieve chest raise, maintain upper airway to aid expiration (eg with SGA).
Surgical cricothyrotomy is suggested if needle cricothyroidotomy fails
Unanticipated Difficult Airway
Common peri-operative critical events in children
Desaturation - due to a combination of increased work of breathing, small FRC (low intrapulmonary O2 reserve), higher basal metabolic rate and diaphragm dependence. Other causes include: - endobronchial intubation, reduced diaphragmatic compliance from stomach inflation, etc
Laryngospasm – due to high parasympathetic tone, most likely during light anaesthesia or vagally stimulating procedures e.g. laryngoscopy or extubation
Bradycardia – due to high parasympathetic tone, most likely during vagally stimulating procedures e.g. laryngoscopy, extubation and squint surgery
Unanticipated Difficult Airway
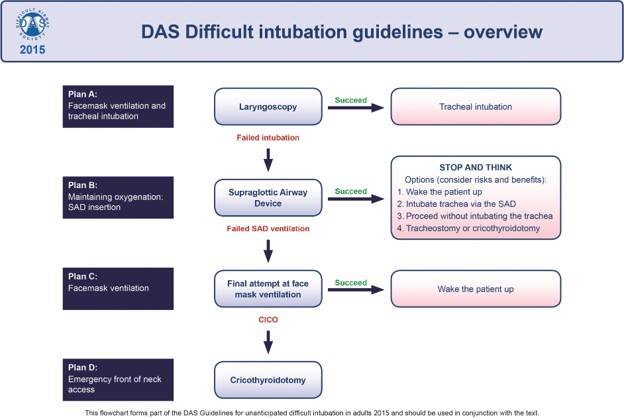
The Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults are used internationally and are familiar to all anaesthetists. To reduce the chance of confusion it is recommended that the same principals are adopted when deployed. The following if the abstract of the reference text taken from https://das.uk.com/guidelines.
"These guidelines provide a strategy to manage unanticipated difficulty with tracheal intubation. They are founded on published evidence. Where evidence is lacking, they have been directed by feedback from members of the Difficult Airway Society and based on expert opinion. These guidelines have been informed by advances in the understanding of crisis management; they emphasize the recognition and declaration of difficulty during airway management. A simplified, single algorithm now covers unanticipated difficulties in both routine intubation and rapid sequence induction. Planning for failed intubation should form part of the pre-induction briefing, particularly for urgent surgery. Emphasis is placed on assessment, preparation, positioning, preoxygenation, maintenance of oxygenation, and minimizing trauma from airway interventions. It is recommended that the number of airway interventions are limited, and blind techniques using a bougie or through supraglottic airway devices have been superseded by video- or fibre-optically guided intubation. If tracheal intubation fails, supraglottic airway devices are recommended to provide a route for oxygenation while reviewing how to proceed. Second-generation devices have advantages and are recommended. When both tracheal intubation and supraglottic airway device insertion have failed, waking the patient is the default option. If at this stage, face-mask oxygenation is impossible in the presence of muscle relaxation, cricothyroidotomy should follow immediately. Scalpel cricothyroidotomy is recommended as the preferred rescue technique and should be practised by all anaesthetists. The plans outlined are designed to be simple and easy to follow. They should be regularly rehearsed and made familiar to the whole theatre team."
The Vortex Approach offers an alternative approach to the unanticipated difficult airway and is based around a “high acuity implementation tool” intended to help clinical teams perform under pressure by providing a simple, consistent template that can be taught to all clinicians involved in advanced airway management. The following text is taken from https://www.vortexapproach.org/.
The Vortex implementation tool is based on the premise that there are only three upper airway 'lifelines' (non-surgical techniques) by which alveolar oxygen delivery can be established and confirmed: face mask, supraglottic airway and endotracheal tube. If a 'best effort' at each of these three lifelines is unsuccessful then a can't intubate, can't oxygenate situation (CICO) situation exists and 'Neck Rescue' (emergency front-of-neck access) must be initiated.
Completion of a 'best effort' at any of the three upper airway lifelines without being able to restore alveolar oxygen delivery mandates spiral movement inward towards the next lifeline. The circular arrangement of the three lifelines on the tool means that airway management can be initiated using any lifeline and proceed to the remaining ones in whatever sequence is judged most appropriate in the clinical circumstances. A list of five categories of optimisation, applying equally to each of the three lifelines, is provided to prompt consideration of the available options for maximising success during a best effort at any lifeline.
Completion of best efforts at all three lifelines without restoring alveolar oxygen delivery culminates in spiral movement to the centre zone of the tool, representing the need to initiate Neck Rescue. Conversely, confirmation of alveolar oxygen delivery using any of the three lifelines, results in outward movement into the circumferential 'Green Zone'. The Green Zone prompts recognition of the opportunity to re-oxygenate, gather resources and develop a strategy, that arises whenever alveolar oxygen delivery is able to be established. The Green Zone is also visible in the centre of the tool to remind clinicians that, when all three lifelines have been unsuccessful, Neck Rescue also restores alveolar oxygen delivery and provides the same opportunities.
Anticipated Difficult Airway
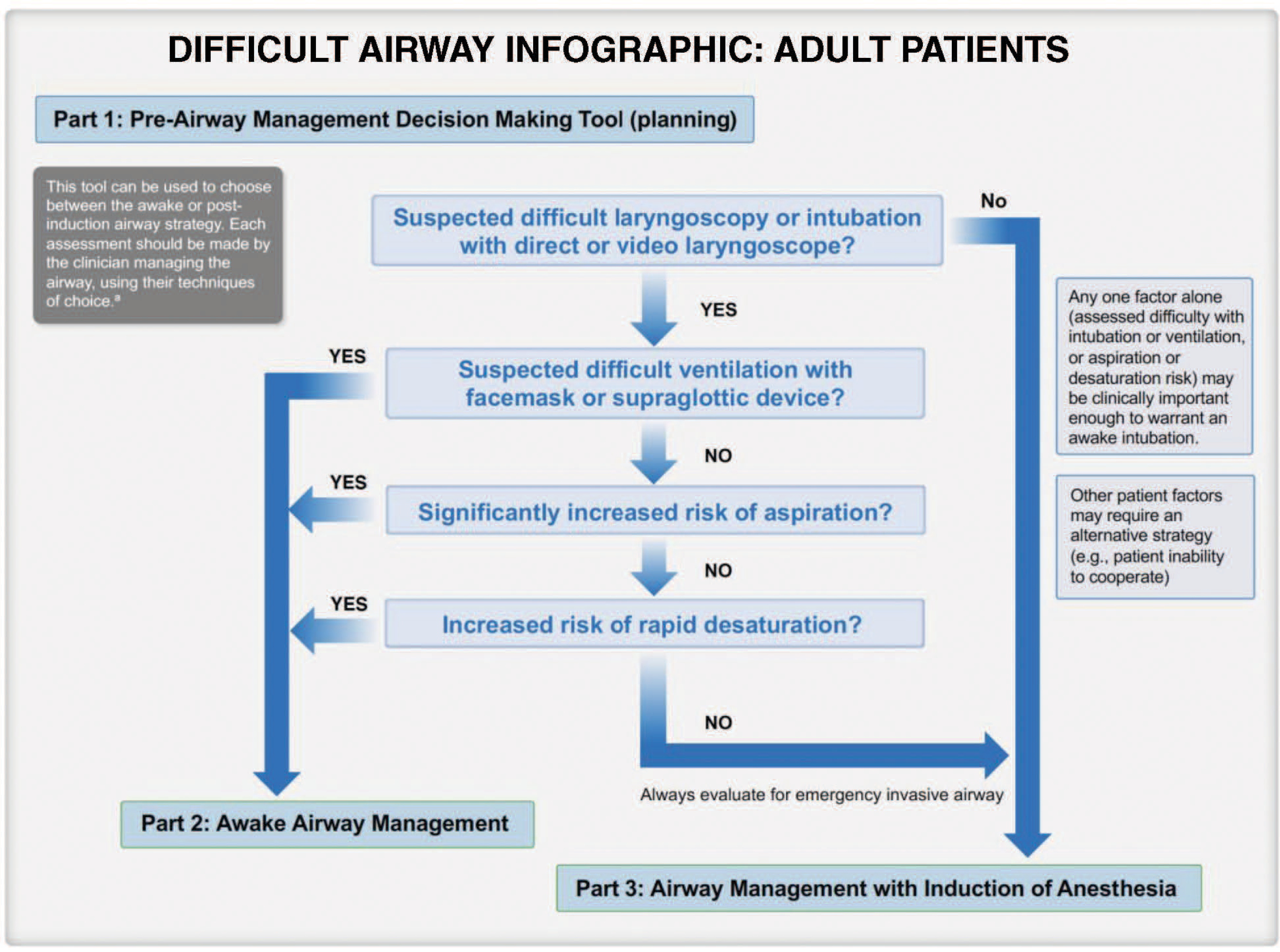
Anaesthesia Patient Safety Foundation Update: 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway - Previous guidelines have been valuable for planning and identifying potential obstacles in developing a difficult airway management strategy. They included questions that helped with decision-making regarding awake airway management. However, judgment errors (i.e., not performing awake intubation when indicated) have led to failed airway securement, according to several reviews.2,3 To further support decision-making, this update includes a decision tree to aid in determining when awake airway management is indicated (Figure 1, Part 1). This decision tree is an extension and evolution of a work product published in 2004 by a task force member and adapted for the 2022 ASA algorithm.4 Awake intubation of the adult patient should be considered when there is (1) difficult ventilation (face mask/supraglottic airway), (2) increased risk of aspiration, (3) intolerance of brief apnoea, or (4) expected difficulty with emergency invasive airway access.
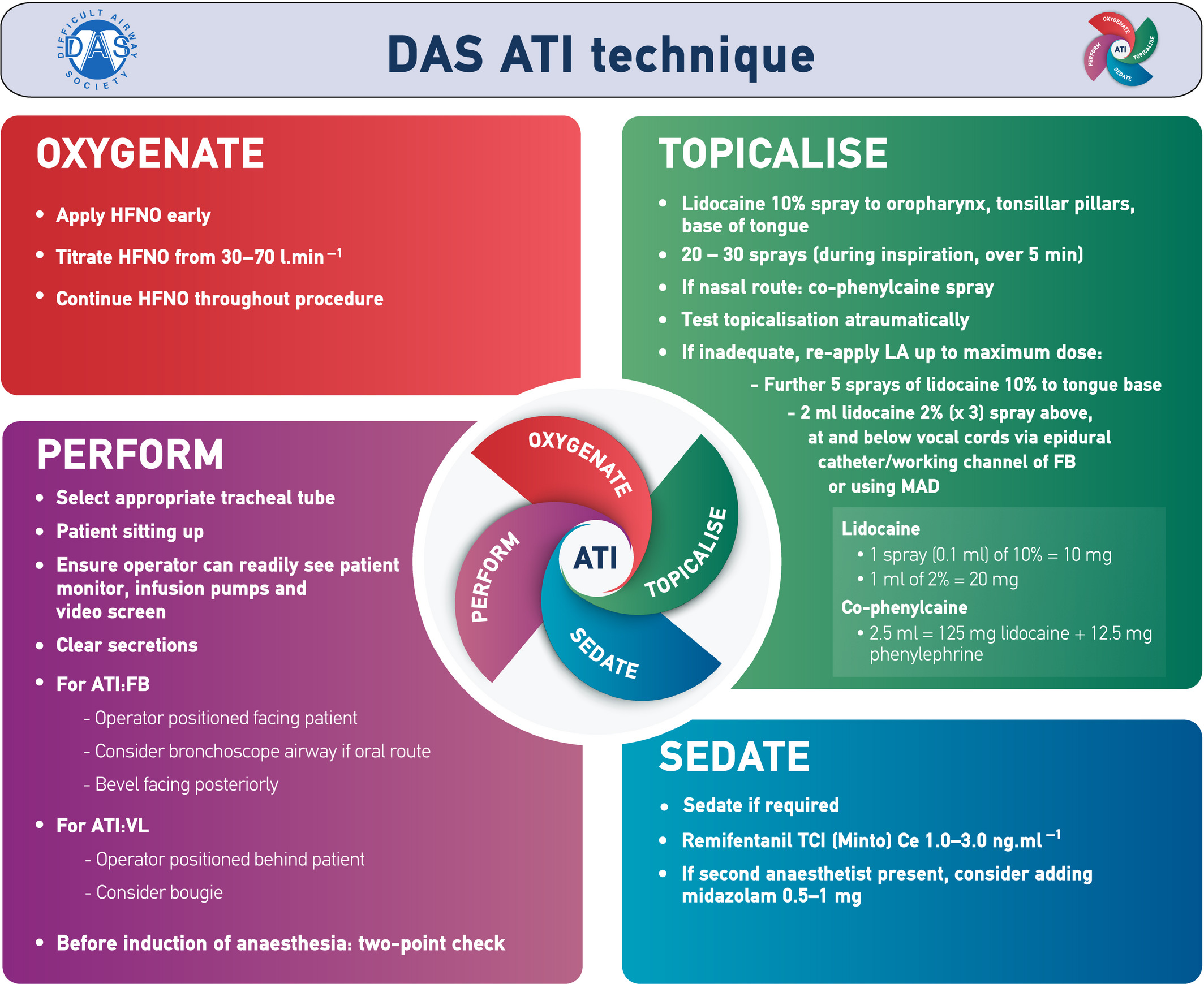
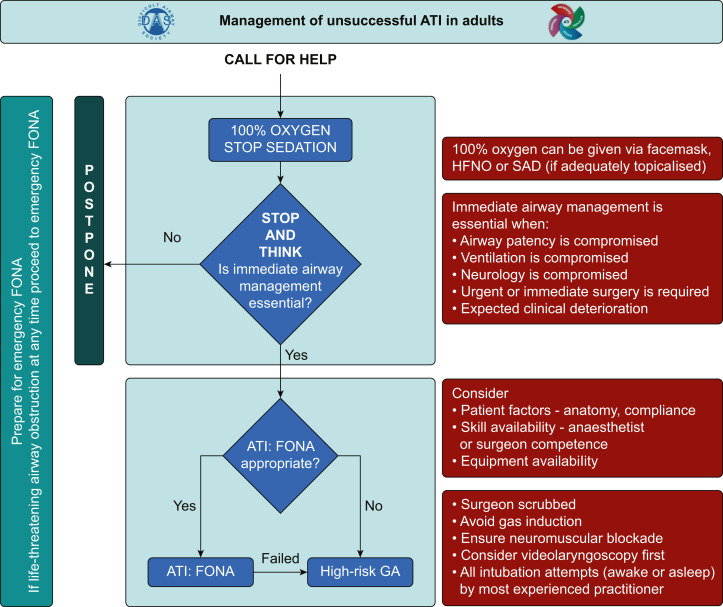
Difficult Airway Society guidelines (2019) for awake tracheal intubation (ATI) in adults. These guidelines aim to support clinical practice and help lower the threshold for performing awake tracheal intubation when indicated. Recommendations:
Awake tracheal intubation must be considered in the presence of predictors of difficult airway management. A cognitive aid such as a checklist is recommended before and during performance of awake tracheal intubation.
Supplemental oxygen should always be administered during awake tracheal intubation.
Effective topicalization must be established and tested. The maximum dose of lidocaine should not exceed 9 mg.kg−1 lean body weight.
Cautious use of minimal sedation can be beneficial. This should ideally be administered by an independent practitioner. Sedation should not be used as a substitute for inadequate airway topicalization.
The number of attempts should be limited to three, with one further attempt by a more experienced operator (3 + 1).
Anaesthesia should only be induced after a two-point check (visual confirmation and capnography) has confirmed correct tracheal tube position.
All departments should support anaesthetists to attain competency and maintain skills in awake tracheal intubation.
Deployed considerations: (DRAFT)
Patient positioning may be challenging, lateral positioning, use of a stretcher backrest or performing the procedure propped up on the floor have been described. Safety following a dynamic risk assessment must be prioritised.
The 7mm ETT is the smallest that can be railroaded over the deployed AMBU scope. An armoured tube is more flexible and may be more resistant to compression / kinking.
Nasal maucosal atomisation devices are available in resus holdings.
Epidural catheters (NR fit) and 3mm NR syringes are available in the FST holdings of the 370
Lignocaine - await update re concentration in 370 holding
Co-phenylcaine - await update re 370 holding
Anaesthesia for Traumatic Brain Injury
Early Recognition of Traumatic Brain Injury
History
Loss of consciousness at any time
Altered mental status
History of seizure
Exposure to blast (particularly if enclosed space)
Any injury above clavicles
Clinical Observations
External head wounds
Decreased GCS
Unequal pupils
Focal neurology
Headache/nausea/vomiting
Seizure activity
[Where available] An Urgent CT head scan should be performed in patients with suggestion of moderate to severe traumatic brain injury (GCS < 13)
Prevention of Secondary Brain Injury
Maintain Airway patency and cervical spine stabilisation
Ketamine is an appropriate induction agent to maintain haemodynamic stability.
In the case of an isolated head injury propofol induction may be preferred.
Maintain PaO2 > 13kPa
Maintain PaCO2 between 4.5 - 5.0 kPa
Hyperventilation in the acute phase is not recommended.
In the presence of brain herniation stigmata, short term hyperventilation to a PaCO2 < 4.0 kPa may be utilised, but only to facilitate other procedures (e.g. transfer to CT).
Maintain MAP > 80mmHg in adults
Cerebral perfusion requires an adequate mean (CPP=MAP-ICP).
Haemostatic resuscitation will mitigate the effect of hypovolaemic shock.
Viscoelastic testing is important as coagulopathy is found in 1/3 of severely head injured patients.
The blood pressure needed to maintain minimum CPP allowing for metabolic needs to be met in children with severe TBI is unknown, suggest maintaining above 75th centile for age.
Manage Intracranial Pressure (ICP)
Venous drainage - Tape ETT tubes, ensure correct sizing of cervical collar, 30° head up (if injury pattern permits)
Cerebral metabolism - ensure adequate anaesthesia and paralysis, treat seizures.
Hypertonic treatment clinical or radiological evidence of brain herniation syndromes (note treatment may temporise but has not been shown to demonstrate improvements in outcome).
10% Mannitol 0.25-1.0gKg-1 to maintain serum osmolarity <320mOsm L-1
5% NaCl 1 - 2mls Kg-1 (beware hyperchloraemia)
Surgery - evacuate clot and stop bleeding
Maintain Haemoglobin at 100gL-1
Control Temperature
Normothermia should be maintained as there is no evidence to support the routine use of hypothermia in TBI.
Pyrexia should be avoided.
Aim for Blood Glucose < 10mmol L-1
Regular monitoring and insulin sliding scale if required.
Seizure control
Treat seizures when they occur, levetiracetam or phenytoin are reasonable choices.
Anaesthesia and airway trauma
A recently published metanalysis has been used as the foundation for this guidance. Airway management in patients with airway injury focuses on maintenance of spontaneous ventilation if at all possible, intubation under direct vision (to avoid the creation of a false passage) and the avoidance of both PPV and cricoid pressure during RSI is recommended. In case of failed intubation surgical tracheostomy is the rescue plan most likely to avoid making the situation worse. When managing burns patients the Difficult Airway Society 2015 guidelines apply.
Consider urgency: no time, some time, or adequate time for airway assessment, investigation, and intervention. If the patient is in extremis and there is no time for assessment, the anaesthetist must manage the patient urgently while planning for the worst-case scenario. Objects that impale the patient should be trimmed carefully so they do not impede subsequent airway interventions. Location is important – where is the safest location to proceed?
Burns
The requirement for intubation is not always clear-cut. History and onward patient course are important factors. Initially burns result in exposure to chemicals and particulates, thermal and blast injuries may also coexist. Subsequent physiological (volume resuscitation, SIRS +/- infection, thermoregulation etc) and nursing demands can be extreme. In case of airway burn anticipate the potential for deterioration, insert a large uncut ETT (to facilitate bronchoscopy and allow for swelling). Lage burn injuries are very dynamic and may progress quickly following fluid resuscitation.
Max Fax trauma
Airway concerns:
Posteroinferior displacement of the fractured maxilla may obstruct a NPA.
Bilateral fracture of the anterior mandible or parasymphysial fracture may cause the tongue to fall back and block an OPA.
Foreign bodies such as fractured teeth, bone fragments, and blood or vomit may block the airway.
Heamatoma due to haemorrhage from major vessels or bleeding from open wounds may contribute to airway obstruction.
Soft-tissue oedema resulting from trauma can cause delayed airway compromise.
Laryngotracheal trauma may cause oedema and displacement of upper airway structures aggravating the risk of cervical airway obstruction.
Suction and positioning are key. The SALAD (suction assisted laryngoscopy airway decontamination) technique, ie placing a suction device in oropharynx may be effective.
Post-intubation packing of the airway to prevent further bleeding.
Anaesthesia for Thoracotomy
Airway Management
Follow conventional <C>ABC with standard RSI anaesthetic and controlled ventilation. It is likely that adequate lung isolation can be achieved with a single lumen endotracheal tube, right sided endobronchial intubation can be achieved by advancing the ETT beyond the cornea, left sided endobronchial intubation may require rotation of the ETT 90 degrees anticlockwise to encourage left sided passage, railroading over a bronchoscope or with manual assistance from a surgeon. Adequate placement can be confirmed by observing chest movement, auscultation or USS; once surgery has started lung movement should be obvious. If a dual lumen tube is desired 37F and 39F left sided disposable tubes are available on the module, if used replacement with a single lumen tube is suggested prior to transfer.
One Lung Ventilation
OLV indications that may be encountered on deployment:
Absolute (enable respiration) - massive haemorrhage / major bronchial disruption
High priority (surgical access) - thoracic surgery
Low priority indications (surgical access) - oesophageal / cardiac surgery
Optimal management of hypoxaemia during OLV requires a thorough understanding of the underlying mechanisms and causes. Besides OLV itself, V/Q matching (largely intrapulmonary shunt) is also influenced by patient position, anaesthesia, cardiac output, mode of ventilation, lung disease and factors that affect hypoxic pulmonary vasoconstriction (HPV). HPV is a biphasic response, starting after a few seconds (plateaus by 30 min) and if hypoxaemia persists a second phase begins at about 40 mins (plateaus after 2 hrs).
Pulmonary vascular resistance and cardiac output are affected by the patient’s metabolic state. The effect of cardiovascular drugs on HPV largely depends on their effect on cardiac output and pulmonary vascular resistance. With modern IV and inhalation anaesthetic agents this does not occur at clinically relevant doses. Alkalosis and hypocarbia increase shunt and should be avoided during OLV. High ventilatory pressures may encourage blood flow to the non-dependent lung, further worsening shunt. Surgical retraction may help by increasing PVR in the operative lung. However, manipulation of lung tissue, through the release of vasoactive substances, may also inhibit HPV. Clamping or ligating the pulmonary artery or its branches in the operative lung reduces blood flow to the non-ventilated lung and improves PaO2.
One lung ventilation in the supine position is generally less well tolerated than in the lateral position. Therefore, shunt through the non-ventilated lung is relatively greater, resulting in worse oxygenation.
Hypoxia during one lung ventilation should be managed in the following manor.
Anaesthesia for resuscitative thoracotomy
This is procedure is an emergency procedure, reserved for patients in Low Output Sate (LOST) or No Output State (NOST). The priorities will depend on presentation, the HOTT (Hypotension, Oxygenation, Tension pneumothorax and Tamponade) mnemonic is a helpful aide-memoire for cardiac (peri-) arrest following trauma. The patients most likely to benefit from a resuscitative thoracotomy are those with cardiac tamponade. Outcomes in patients who have had a cardiac arrest following exsanguination are poor.
Induction of anaesthesia (if required) should be in accordance with the above guidance, a single lumen tube should be used. Concurrent and aggressive resuscitation is essential if the procedure is deemed appropriate. ROSC can be rapid following release of a tamponade and consideration should be given to worsening arterial bleeding secondary to surgery and also return of consciousness.
Anaesthesia for Myocardial Repair
Patient positioning
Move operating table to aid surgical exposure and temporarily increase pre-load
Use rotation and Trendelenburg to minimise retraction/rotation of heart
Access to the lateral LV will require rotation with patient right side down with 20-30° head down
Be prepared to pause ventilation to aid surgical access
Communicate with Surgeon
Ensure pericardium is opened maximally
Ensure sutures are used to elevate the pericardium (not swabs)
Surgical manipulation may lead to hypotension or loss of cardiac output with transient arrhythmia. Stop or reduced manipulation and allow restoration of output
Inotropes and Rate Control
Aim for HR 60 - 75 and accept transient hypotension to allow surgical repair.
Consider Esmolol or Neostigmine to slow heart rate (or Adenosine for temporary arrest)
Avoid inotropes and/or accept lower BP post repair
Postoperative care after pulmonary or bronchial injury
Principles of Postoperative care include:
Avoid positive pressure ventilation
Excellent analgesia is key
Involve physiotherapy early
Avoid over-transfusion and over-hydration
Last reviewed:
23/01/2026
Next review date:
23/01/2027
Related resources
Wiles, Matthew D., et al. "Airway management in patients with suspected or confirmed cervical spine injury: Guidelines from the Difficult Airway Society (DAS), Association of Anaesthetists (AoA), British Society of Orthopaedic Anaesthetists (BSOA), Intensive Care Society (ICS), Neuro Anaesthesia and Critical Care Society (NACCS), Faculty of Prehospital Care and Royal College of Emergency Medicine (RCEM)."Anaesthesia 79.8 (2024): 856-868.
Hagberg, C.A., Gabel, J.C. and Connis, R.T., 2015. Difficult Airway Society 2015 guidelines for the management of unanticipated difficult intubation in adults: not just another algorithm.BJA: British Journal of Anaesthesia,115(6), pp.812-814. DAS Intubation Guidelines (2015)
Bourn S, Rylah O, Fishenden T, et al. Diamedica Draw-over Vaporiser: bench testing the UK Defence Anaesthesia System in the deployed environment. BMJ Mil HealthPublished Online First: 11 June 2024. doi: 10.1136/military-2023-002652
Richards ND, Weatherhead W, Howell S, Bellamy M, Mujica-Mota R. Continuous infusion ketamine for sedation of mechanically ventilated adults in the intensive care unit: A scoping review. Journal of the Intensive Care Society. 2023;25(1):59-77. doi:10.1177/17511437231182507
Sellers, C. et al. Inhalational induction in paediatric anaesthesia, BJA Education, Volume 23, Issue 1, 32 - 38
Frerk, C., Mitchell, V.S., McNarry, A.F., Mendonca, C., Bhagrath, R., Patel, A., O'Sullivan, E.P., Woodall, N.M. and Ahmad, I., 2015. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults.BJA: British Journal of Anaesthesia,115(6), pp.827-848.
Apfelbaum, J.L., Hagberg, C.A., Connis, R.T., Abdelmalak, B.B., Agarkar, M., Dutton, R.P., Fiadjoe, J.E., Greif, R., Klock, P.A., Mercier, D. and Myatra, S.N., 2021. 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway.Anesthesiology,136(1), pp.31-81.
Shum, S., Huang, A. and Slinger, P., 2023. Hypoxaemia during one lung ventilation.BJA education,23(9), pp.328-336.