Tachyarrhythmia
Warning
Objectives
To guide the management of patients presenting to medical facilities with tachyarrhythmia.
Scope
This guideline describes the resuscitation of patients with tachyarrhythmia in the emergency setting. It also considers Prolonged Casualty Care and Paediatric circumstances. There are separate guidelines for managing stable patients presenting with new tachyarrhythmias such as atrial fibrillation (AF) or atrial flutter.
Audience
This guideline is intended for the use of registered healthcare professionals fulfilling a general role in forward medical locations or in an Emergency Department on deployed operations.
Initial Assessment & Management
Tachyarrhythmia is likely to be a rare occurrence in a population of young, healthy, pre-screened Service Personnel. However, it may still be encountered on operations due to undiagnosed cardiac conditions, intercurrent illness, allied nation forces or amongst civilian populations.
MARCH Assessment
Rapid Primary Survey
Monitor ECG, BP, SpO2
Record 12-lead ECG if available: circumstances may dictate that treatment decisions are made with a 3-lead ECG or defibrillator pad single lead.
Give oxygen if SpO2 <94%
Obtain IV access
Identify and treat reversible causes:
- Electrolyte abnormalities - medications (e.g. diuretics), fluid loss (vomiting/diarrhoea/sweating), pre-existing conditions (renal disease, diabetes) or nutritional deficiency.
- Appropriate secondary physiological response to another illness? E.g. sepsis, ACS, PE, trauma
Life threatening features → Unstable Pathway
Shock - systolic blood pressure <90mmHg or unrecordable, impalpable radial pulses, decreasing level of consciousness, pale, clammy appearance
Syncope - transient loss of consciousness not otherwise explained.
Myocardial ischaemia - cardiac chest pain, ECG changes e.g. widespread ST depression, ST elevation
Severe heart failure - respiratory failure, pulmonary oedema.
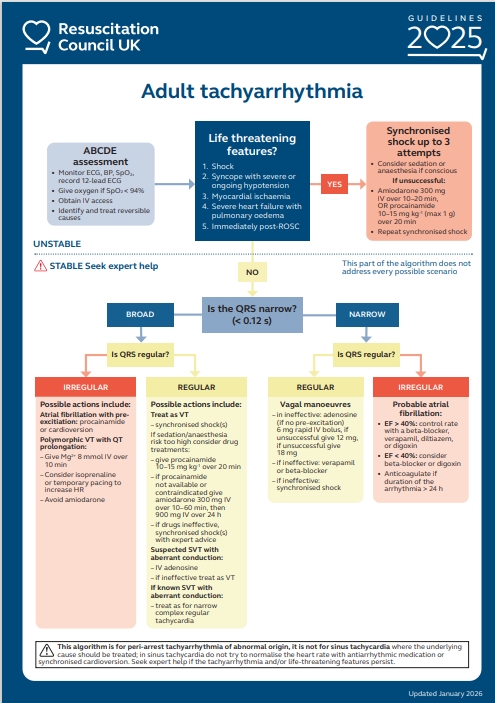
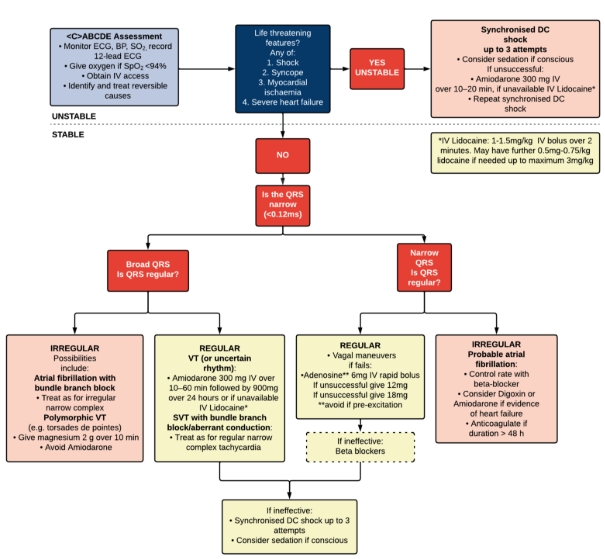
If there is evidence of life-threatening features immediate Synchronized Direct Current Cardioversion (DCCV/DC Shock) should be performed.
Stability/instability is a spectrum — if in doubt, perform Synchronized DCCV.
Synchronised Shock
Up to 3 attempts
Ensure shocks are delivered in synchronized mode – confirm prior to each shock delivered
Ensure correct pad placement - use antero-lateral or antero-posterior pad placement.



Recommended energy of shocks:
- Atrial fibrillation - deliver at the maximum available energy
- Atrial flutter/SVT - 100J with stepwise escalation with further shocks
- Ventricular tachycardia - 150J with stepwise escalation
Consider sedation or anaesthesia if patient is conscious (choice of pharmacological agents according to the skill set of the practitioner and capability of the medical treatment facility).
If at any point the patient loses cardiac output, change to Advanced Life Support protocols
If unsuccessful after 3 Synchronised shocks:
- Amiodarone 300mg IV over 10-20 minutes or Lidocaine 1-1.15mg/kg IV bolus over 2 minutes (further lidocaine boluses of 0.5-0.75 mg/kg up to a maximum of 3mg/kg can be used) - amiodarone can still be administered following administration of lidocaine
- Attempt to optimize physiology and correct any electrolyte abnormality
- Repeat synchronized DCCV
- Maximum recommended energy
- Change pad position
Successful cardioversion should be demonstrated by restoration of sinus rhythm and improvement in haemodynamic function. Overdrive pacing or cardiology opinion via clinical reachback can be considered if the tachyarrhythmia remains and the patient is unstable.
No life-threatening features → stable pathway
Broad or Narrow?
Is the tachyarrhythmia broad or narrow complex?
- Narrow complex is defined as a QRS <120ms (3 small squares on standard ECG).
- Broad complex is defined by QRS >120ms.
Tachycardia is further differentiated into regular or irregular.
Broad Complex Tachyarrhythmias
Regular or Irregular?
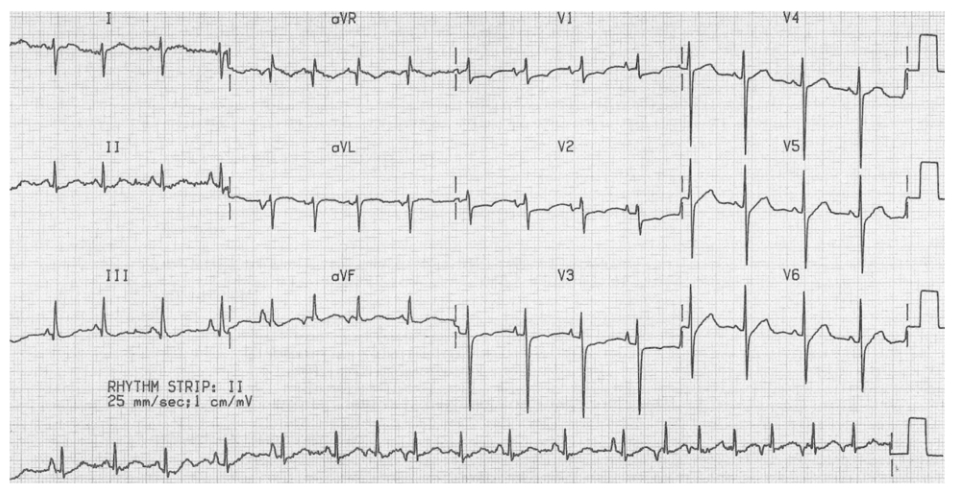
Regular:
The most common cause of Regular Broad complex Tachycardia is ventricular tachycardia (VT).
High risk arrhythmia.
More likely with a history of ischaemia, structural heart disease and prior MI.
Place defibrillator pads pre-emptively
First line treatment (stable pathway):
Amiodarone 300mg IV over 10-60 minutes followed by an infusion of 900mg over 24 hours. Amiodarone loading doses can drop BP if given too quickly. For the 24-hour infusion of amiodarone reliable IV access should be ensured as extravasation can be highly injurious
Or Lidocaine 1-1.15mg/kg IV bolus over 2 minutes (further lidocaine boluses of 0.5-0.75 mg/kg up to a maximum of 3mg/kg can be used)
Second line treatment (stable pathway):
Synchronised DC shock, with procedural sedation or anaesthesia as appropriate for practitioner skill set in the conscious patient.


Less common causes are:
- SVT with bundle branch block (sometimes called SVT with aberrant conduction )
- Sinus Tachycardia with bundle branch block
See Narrow Complex- regular pathway
Assess and manage underlying cause
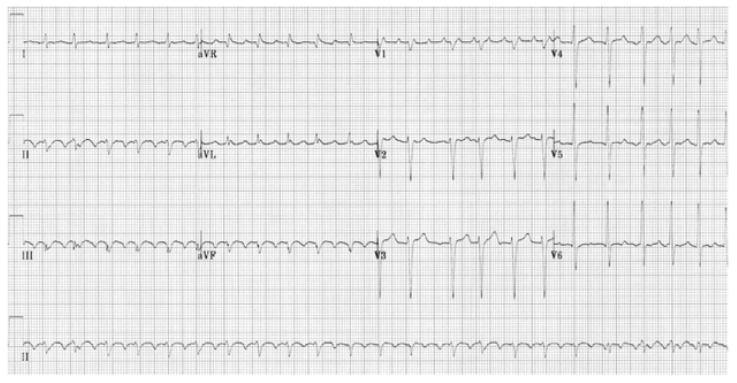
Irregular:
The most common causes of Irregular Broad complex tachycardia are:
- Atrial fibrillation with bundle branch block
- Polymorphic ventricular tachycardia (Torsades de Pointes)
Atrial fibrillation (AF) with a bundle branch block
- Reasonably benign
- Pre-existing bundle branch block
- Irregularly irregular monomorphic complexes
- See Narrow complex – irregular pathway
Polymorphic ventricular tachycardia with prolonged QT interval (Torsades de pointes)
Continuously changing amplitude
Rapid, irregular QRS complexes twisting around baseline
Associated with prolonged QT syndromes, electrolyte imbalance (hypomagnesaemia/hypokalaemia).
Often transient and intermittent
First Line Treatment:
- Magnesium 2g IV over 10 minutes (if available)
- Correct other electrolyte disturbance
- Avoid Amiodarone (increases QT interval)
- If above measures fail, synchronised DC shock
- If failure to discharge as defibrillator does not recognise complexes and the patient becomes unstable, administer an unsynchronised shock.

Narrow Complex Tachyarrhythmias
Regular or Irregular?
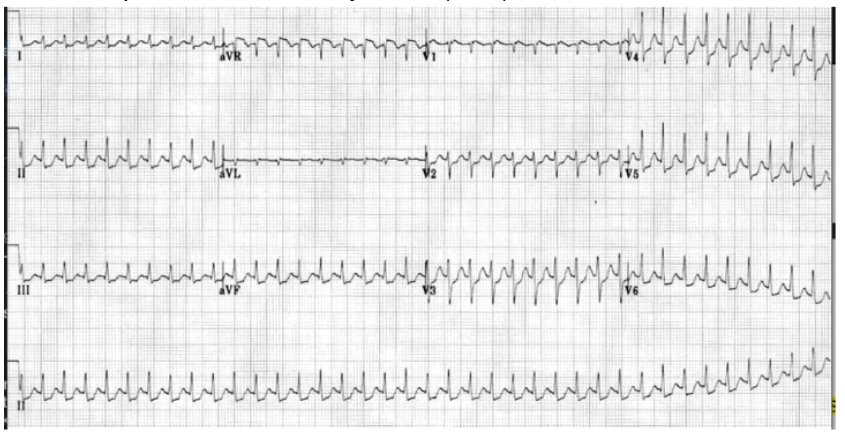
Regular narrow complex:
The three most common causes of a regular narrow complex tachycardia are:
- Sinus tachycardia
- Atrial Flutter
- Supraventricular tachycardia (SVT)
Sinus tachycardia
Assess and manage underlying cause
Do not attempt to normalize the heart rate with antiarrhythmic medication or synchronized cardioversion
Atrial Flutter
Can be managed either as per Irregular Narrow Complex (AF) pathway or if diagnostic uncertainty as per SVT management below.
SVT
First Line management
Vagal manoeuvres
Modified Valsalva (two-person technique):
Sit the patient in the semi-recumbent position at 45 degrees, encourage to Valsalva by forced expiration into a syringe for 15-20 seconds.
At the end of this expiration phase, lay the patient flat whilst an assistant raises the legs to 45 degrees without delay, hold this position for 15 seconds
Reverse Valsalva manoeuvre. The patient exhales without force, pinches their nose and closes their mouth tightly before inhaling against resistance for 10 seconds
Second line management, if vagal manoeuvres ineffective:
Adenosine
6mg rapid IV bolus
If unsuccessful, 12 mg rapid IV bolus
If unsuccessful, 18mg rapid IV bolus
Adenosine should be avoided in patients with pre-excitation syndrome e.g. Wolff Parkinson White syndrome, heart block and sick sinus syndrome
Response to Adenosine can be diagnostically useful e.g. in differentiating SVT from atrial flutter
No response at all, likely inadequate dose or delivery
If rhythmic flutter waves revealed, treat as per AF pathway
Temporary reversal to sinus rhythm followed by return to SVT despite maximum dose of adenosine, rate control should be instituted as per AF pathway.
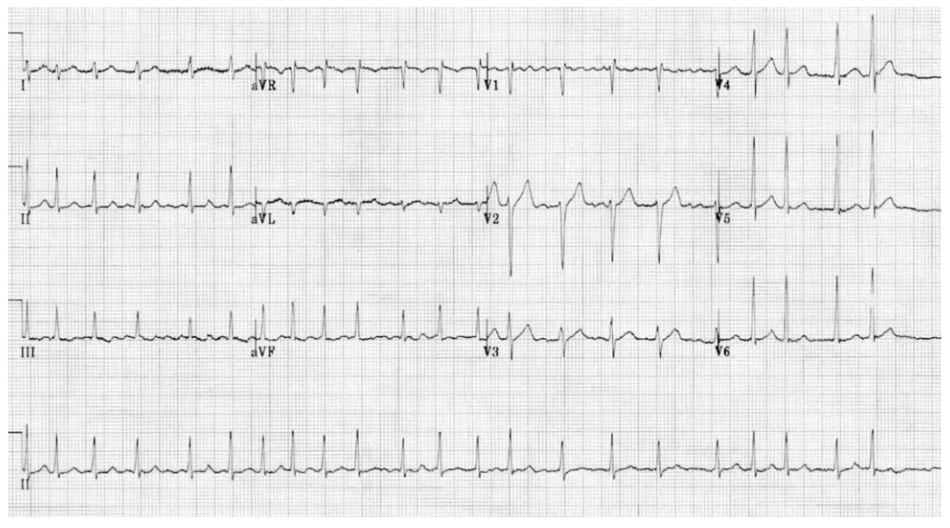
Irregular narrow complex
The three main causes are:
- Atrial Fibrillation
- Atrial flutter with variable block
- Multifocal Atrial Tachycardia

Management of Irregular Narrow Complex Tachycardia
Consider if this is Primary or Secondary tachyarrhythmia
Assess and manage any underlying cause (e.g. sepsis, electrolyte disturbance, caffeine overuse, stimulant drug use, thyrotoxicosis, alcohol excess)
Treatment of reversable causes is often adequate in itself and the majority of patients (~70%) with acute AF will return to sinus rhythm within 48 hours
Secondary AF/Flutter/Atrial tachycardia:
Treat reversible causes and re-assess
If the patient becomes or remains unstable, consider reverting to the unstable tachyarrhythmia pathway or carefully consider the below options
Caution: treating a secondary tachyarrhythmia with rate/rhythm control increases the risk of an adverse event by six times. Take care to exclude underlying causes before treating as primary tachyarrhythmia.
Primary AF/Flutter
- Control rate:
- Unsure of time of onset, chronic AF/Flutter or rhythm-control strategy unsuitable
- Oral Bisoprolol (e.g. 2.5-5mg)
- Oral or IV digoxin (e.g. 500mcg loading dose)
- Unsure of time of onset, chronic AF/Flutter or rhythm-control strategy unsuitable
- Control rhythm
- Acute onset within 48 hrs, rhythm control can be considered
- Chemical cardioversion: amiodarone 300mg IV over 30-60mins
- Electrical cardioversion: synchronised DC shock with procedural sedation or anaesthesia
Consider Anticoagulation if duration from onset of symptoms or ECG evidence of AF >48 hrs
- Carry out AF Stroke risk assessment (CHA2DS2VASc score) and bleeding risk score (e.g. HASBLED or ORBIT)
Anticoagulation is routinely with Apixaban 5mg BD or therapeutic dose Enoxaparin as an alternative
For further management of Atrial Fibrillation outside of the emergency setting, see the Atrial Fibrillation CGO.
Advanced Assessment & Management
As per initial assessment and management.
Prolonged Casualty Care
Polymorphic Ventricular Tachycardia
Refractory Polymorphic VT
Magnesium: If an initial magnesium bolus is unsuccessful, it can be followed by an infusion of 1-4g/hr (4-16 mmol/hr) to target a magnesium level of 1.5-2 mmol/l
Reducing risk of recurrence: increasing the HR shortens the QT interval and reduces the chances of pVT occurring. E.g. dobutamine or adrenaline infusion. In extremis, electrically using transcutaneous pacing:
Rates of 90-110 are likely to be sufficient however up to 140 may be necessary to achieve suppression.
Supraventricular Tachycardia
Refractory SVT
If following maximum Adenosine dose and synchronized DC cardioversion SVT remains, attempt rate control.
First line: Bisoprolol e.g. 2.5-5mg
Second line (if IV required or bisoprolol unsuccessful): Digoxin e.g. 500mg IV/PO
Refractory tachycardia
Reconsider the diagnosis - is this a sinus tachycardia?
Atrial Fibrillation
See Atrial Fibrillation CGO
Paediatric Considerations
There are differences in the prevalence of different dysrhythmias compared with adults. Of note, atrial fibrillation and ventricular tachycardia are much less common in children.
Life threatening features specific to paediatric population:
An absent brachial pulse
Prolonged central capillary refill time
Hepatomegaly as a manifestation of heart failure
BP <5th centile for age:
1 month - 50 mmHg
1 year - 70 mmHg
5 years - 75 mmHg
10 years - 80 mmHg
Synchronised DC Shock
1st Shock: 1 J/kg
2nd Shock: 2 J/kg
3rd, and subsequent shocks: 4 J/kg
Should intravenous access be difficult to achieve and procedural sedation required, consider intramuscular/intranasal agents such as ketamine.
Vagal manoeuvres - for very young children unable to participate in deliberate valsalva manoeuvres you can elicit a diving reflex using a large bag of ice mixed with water and resting this across the child’s face for 15 seconds. Alternatively immerse the face in ice cold water for 5 seconds.