The app and website was publicly released on 2 Apr 2024
Update Jan 2025
The content continues to undergo review by all our cadres.
The content remains subject to the following provisos: - The content will be subject to continuous update and review - Old content (from previous CGOs) will be converted into the new format, using the new tools and layouts - Content may be moved around - The layout will change and reflect the needs of the user - Content will be created - Content may be deleted/retired
CGO development will continue.
Saf [Updated 21 Jan 2025]
Transcutaneous Pacing
!Warning
Objectives
To guide the management of patients presenting to medical facilities who require external transcutaneous pacing.
Scope
This guideline describes the indications for transcutaneous pacing including details of the steps to be followed when using the Tempus Pro device.
Audience
This guideline is intended for the use of registered healthcare professionals fulfilling a general role in a forward medical location or in an Emergency Department on deployed operations.
Indications
Patients who are found to have bradycardia despite treatment of reversible causes with any of the following adverse features who have not responded to atropine as per the CGO for Bradycardia
Shock
Syncope
Myocardial ischaemia
Heart failure
Preparation
Monitor patient using 3 lead ECG, blood pressure, and oxygen saturation.
Place defibrillator pads in either anteroposterior or anterolateral positions on clean, dry skin. You may need to shave any excess hair from the chest to obtain good contact.
Pads may be placed either in the anteroposterior position (as illustrated) or in the conventional anterolateral position that would normally be used for defibrillation. Limited evidence suggests that pacing capture is more likely to be achieved with anteroposterior pad positioning so this is recommended as the initial approach if possible.
Administer sedation and analgesia if the patient is conscious, due to the potential discomfort of pacing.
A recommended approach to analgesia is to administer IV paracetamol and then titrate small doses of intravenous opiate analgesia - for example aliquots of 1-2mg morphine.
If this is not sufficient to manage discomfort, or if the patient is anxious or distressed, then consider conscious sedation - midazolam at a dose of 1mg IV for adults titrating upwards by 0.5mg increase every 2 minutes until desired effect, would be an adequate sedation choice due to its cardiovascular stability and amnesic effects. Follow guidance in the sedation CGO (link to follow) including adequate monitoring and completion of a sedation checklist.
Procedure
Set the pacemaker to the appropriate mode. In the deployed context, fixed-rate mode is generally recommended unless there is a specific need for demand mode.
Demand mode means that the pacemaker is automatically inhibited if a spontaneous QRS complex is detected, but movement artefacts can mimic QRS complexes and inhibit pacing. The Tempus LS defaults to fixed-rate mode.
Set the pacing rate (typically at 70 bpm for an adult patient)
Set energy output to zero or to the lowest available value
Start pacing
Gradually increase until electrical capture is achieved - indicated by electrical spikes followed by QRS complexes. This will typically be between 50-100mA in adults.
Fig 2: Appearance of pacing spikes on ECG
Confirm that electrical capture corresponds to physiological capture by palpation of a central pulse. If no pulse is felt then the apparent electrical activity may be artefactual.
Adjust output to 10-20% (~10mA) above the capture threshold to ensure output is not lost with movement.
The capture threshold is the lowest energy level at which electrical and physiological capture is achieved. A reasonable approach is to turn the energy up until electrical and physiological capture is achieved, then slowly turn it down until capture is lost - this will be the capture threshold. Once identified, set the energy level to 10-20% above this.
Post-Procedure
Consider need for alternative or ongoing analgesia/sedation, especially if pacing has been initiated urgently and analgesia has not already been administered.
Seek specialist advice - transcutaneous cardiac pacing is a temporary measure so evacuation to a higher level of care will be needed.
It may be necessary to use a higher energy level during transfer to reduce the risk of capture being lost - but this is likely to increase the patient's analgesic and/or sedation needs.
Prolonged Casualty Care
Patients requiring transcutaneous pacing should be evacuated to a higher level of care as soon as possible. If evacuation is delayed then seek specialist advice, if possible, to guide ongoing care.
If prolonged sedation is required, do not forget to also optimise analgesia - adequate control of pain will allow for shallower and safer sedation.
Closely monitor blood pressure as a marked of adequate perfusion: if appropriately skilled and equipped then invasive arterial monitoring would be useful (see separate CGO - link to follow).
Burns to the chest wall can be associated with prolonged transcutaneous pacing - if this occurs then place new pads occurring under existing pads, then new pad placement can be considered if ongoing transcutaneous cardiac pacing is required.
Paediatric Considerations
Lower Thresholds: Children might require lower pacing energy due to their smaller body size. Start at 0J with children and work upwards as per adults, but anticipate a likely lower capture threshold.
Rate Adjustments: Pacing target heart rates should be age-appropriate - the target heart rate in an adult is typically 70bpm; see paediatric age per page guide (link to follow) for normal age range heart rate and target accordingly.
Sedation Needs: Children often need deeper sedation and analgesia to manage pacing discomfort. Midazolam can be used at 0.05mg/kg as per the page for age guideline.
Electrode Size & Placement: smaller paediatric-sized pads are unlikely to be available - use the anteroposterior position to ensure pads are not touching and optimise energy delivery to the myocardium.
Close Monitoring: Paediatric patients are more susceptible to metabolic imbalances, which can impact pacing efficacy. Check and treat metabolic derangement if resources allow.
Pacing on Tempus LS
From the home screen, select "Start Pacer".
In order to enable the pacer function, both 3 lead ECG monitoring and pads need to connected as shown.
Once the patient is connected to the monitor, the pacing control buttons will be enabled. Increase the rate to an appropriate level (typically 70 bpm for an adult patient).
The Tempus LS will default to fixed pacing mode unless set to demand mode.
As soon as the current is increased above 0mA, the device will begin pacing. A flashing lightning bolt will appear as illustrated.
Increase current until both electrical and physiological capture is achieved. Identify the capture threshold and set to 10-20% or approx 10mA above capture threshold.
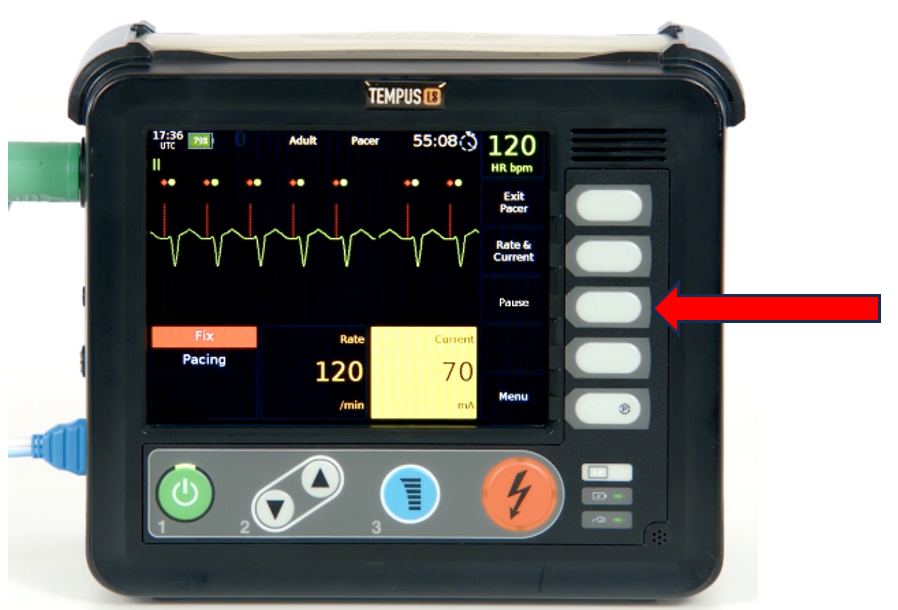
To pause pacing go back to the pacing menu and select the pause button as shown. If "exit pacer" is selected then the device will automatically cease pacing.