Initial Management
Forearm fractures are commonly the result of a high-energy mechanism. Skin should be assessed carefully for open fracture.
The radius and ulnar are mechanically linked, and as such it is important to consider that both bones may be fractured at different levels – carefully examine along the length of the forearm, including the wrist and the radial head to assess for associated injuries. For initial management it should be assumed that both bones are fractured and managed as such.
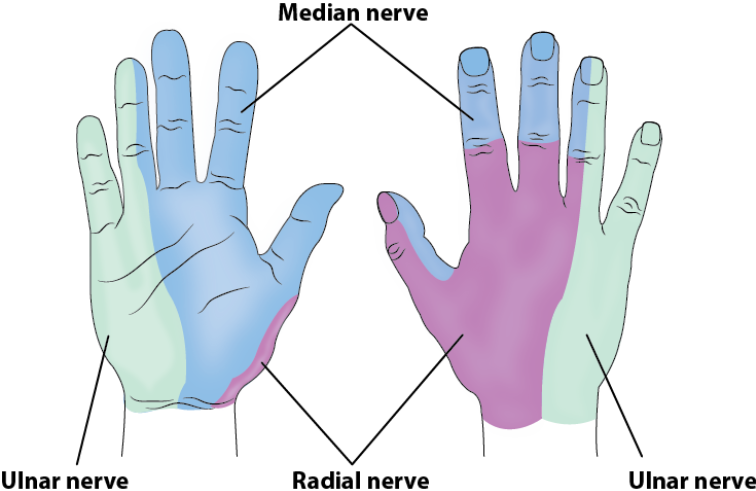
Neurovascular Status: Assess and document motor and sensory function of the radial, median and ulnar nerves Palpate and document the presence of both radial and ulnar pulses and check capillary refill time of the fingers. Assess for compartment syndrome
Reduction: Visible forearm deformity should be reduced to anatomical alignment prior to immobilisation
Immobilisation: SAM splint immobilisation from the metacarpal heads to the upper arm. Elbow in flexion.
Advanced Assessment and Management
As per initial management
Advanced assessment should include consideration of specific injury patterns with management varying based on the injury pattern identified. Forearm fractures have an increased risk of compartment syndrome, and this must be considered and assessed for.
Imaging: X-Ray Forearm (AP and Lateral). Ensure elbow and wrist are included on imaging. Request joint specific x-rays if required
Isolated Radial Shaft Fracture: Carefully examine the distal radio-ulnar joint to assess for associated injury
Galeazzi Fracture-Dislocation: Radial shaft fracture with disruption of the distal radio-ulnar joint. Definitive management is surgical.
Isolated Ulnar Shaft Fracture: Carefully examine the radial head to assess for associated injury
Monteggia Fracture-Dislocation: Proximal ulnar fracture with associated radial head dislocation. Definitive management is surgical
Both-bones Forearm Fracture: Often a high energy injury with high risk of open fractures and compartment syndrome. Definitive management is surgical
Immobilisation: Above elbow backslab with collar and cuff. Ensure careful reassessment of neurovascular status after POP application and monitor for signs of compartment syndrome
In-Theatre Specialist Assessment: required if any of:
- Open fracture / Neurovascular compromise
- Severe displacement or failure of non-invasive immobilisation
- Compartment syndrome